
For localized, mechanical spinal pain exacerbated by backward bending or twisting, choose a facet joint injection. For radiating pain, numbness, or weakness that travels down the leg or arm—often caused by a herniated disc or spinal stenosis—choose an epidural injection. Facet joint injections target the small, stabilizing joints connecting each vertebra, addressing localized osteoarthritis or mechanical wear. In contrast, epidural injections target the epidural space surrounding the spinal cord and nerve roots, delivering anti-inflammatory agents to soothe compressed or irritated nerves. Clinicians frequently use diagnostic facet blocks to isolate joint-specific pathology before considering long-term options like radiofrequency ablation. Meanwhile, epidural steroid injections serve as a primary non-surgical intervention to reduce radicular symptoms and avoid invasive decompression surgery. Choosing between these interventions depends on whether the pain pathology is mechanical (facet-mediated) or neuropathic (nerve root-mediated). A precise clinical diagnosis, verified through physical examination and advanced imaging, determines the optimal therapeutic pathway.
Key Takeaways
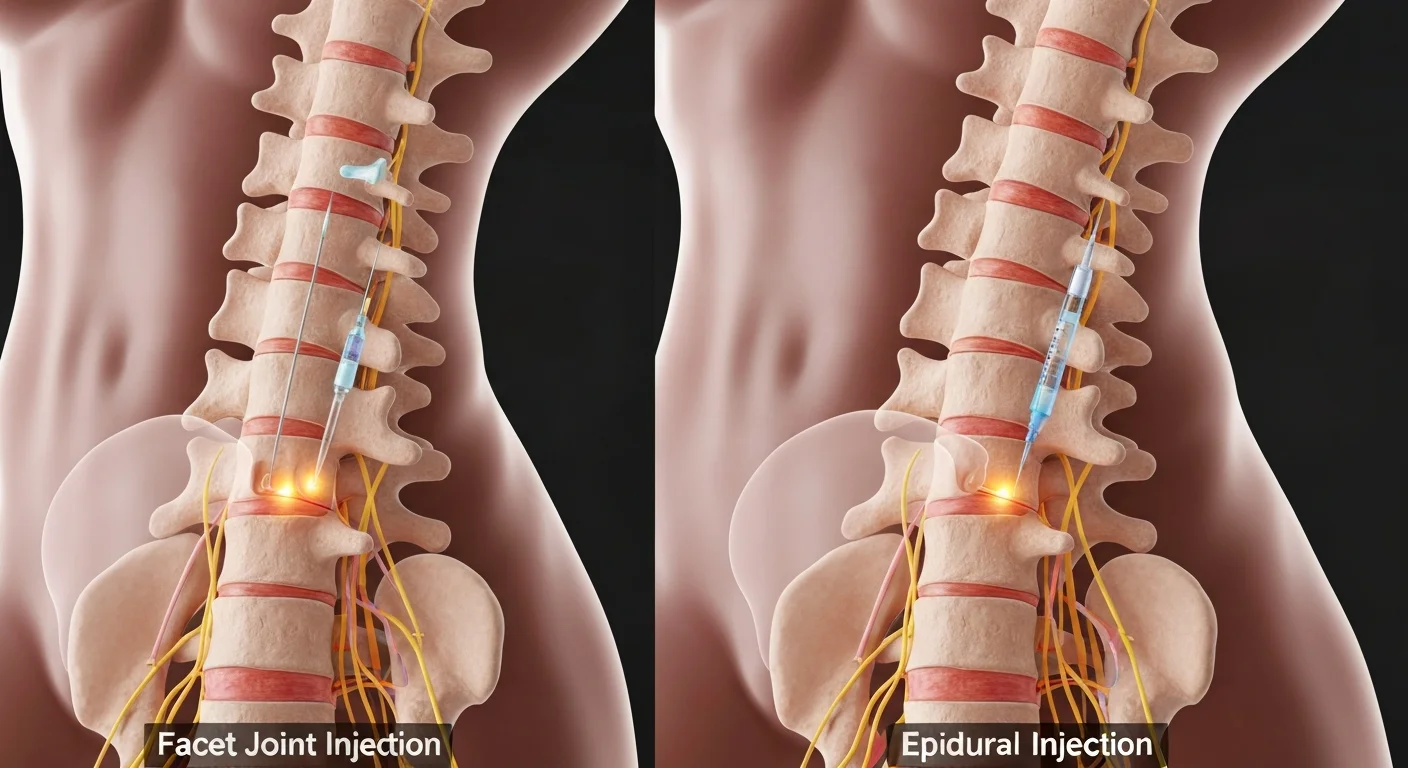
- Facet injections treat localized, mechanical back or neck pain arising from arthritic facet joints, whereas epidurals treat radiating, neuropathic pain (radiculopathy) originating from compressed spinal nerves.
- The injection targets differ: facet injections deliver anesthetic and corticosteroids directly into or around the joint capsule, while epidural injections place medication into the epidural space surrounding the spinal nerves.
- Facet interventions often serve a dual diagnostic-therapeutic purpose, whereas epidural interventions focus primarily on therapeutic inflammation reduction to manage acute or chronic nerve compression.
- Anatomical assessment via fluoroscopic X-ray guidance is mandatory for both procedures to ensure safety, minimize complications, and guarantee precise pharmacological delivery.
- Healthcare providers use these minimally invasive procedures to defer or completely avoid major spinal surgeries, often combining them with targeted physical therapy.
Anatomical Differences Between Facet Joint Injection vs Epidural Injection
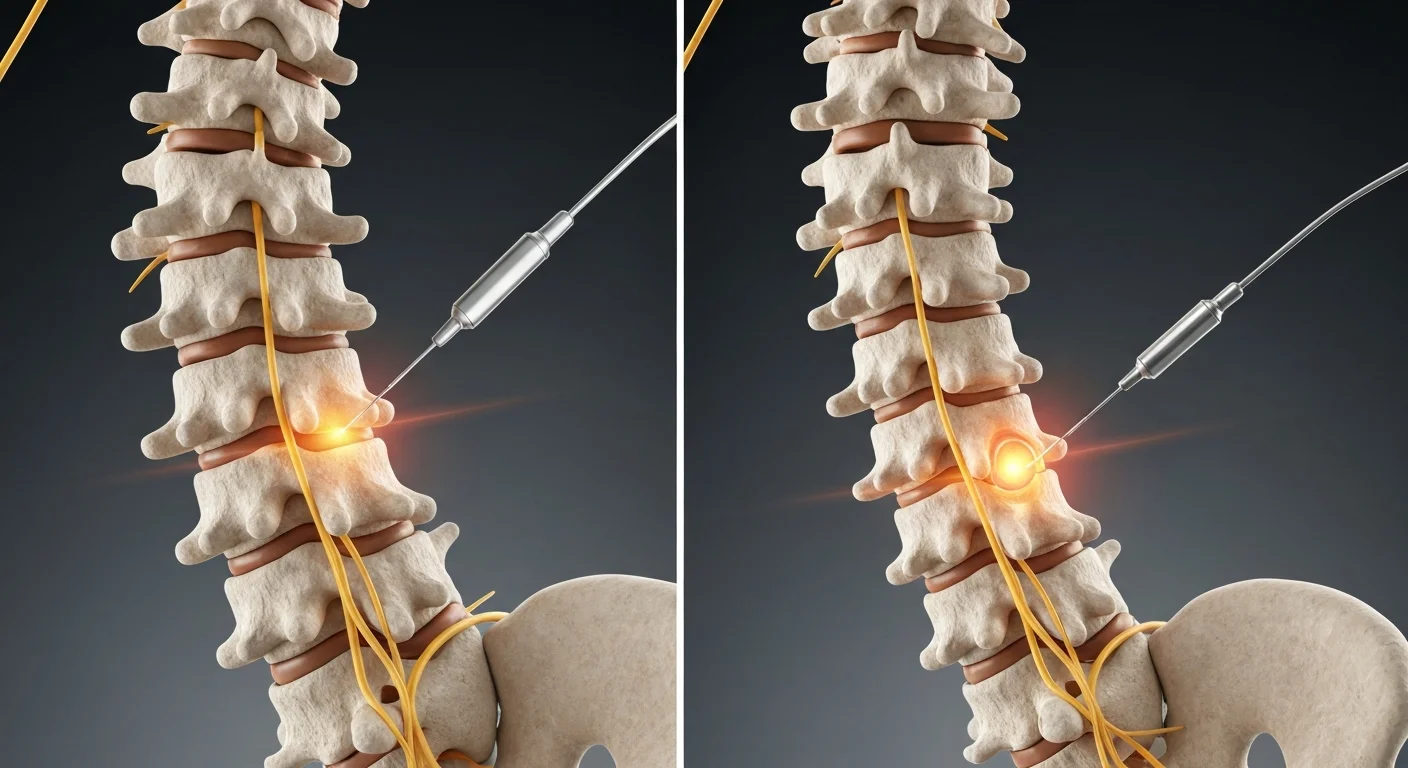
Understanding the structural anatomy of the spine is critical to distinguishing between a facet joint injection and an epidural injection. The human spine consists of 33 vertebrae stacked vertically. These bones connect at the rear of the spine via pairs of small joints called facet joints. These joints, or zygapophysial joints, provide stability and allow the spine to bend and twist. They have a coating of articular cartilage and are enclosed in a synovial membrane. This membrane can become inflamed due to wear, tear, or systemic arthritis, which is similar in diagnostic utility to a facet block procedure.
In contrast, the epidural space is a distinct anatomical zone within the spinal canal. It is the outermost sleeve of the spinal cord’s protective covering. The epidural space sits outside the dura mater, the thick membrane protecting the spinal cord. It contains fat, blood vessels, and nerve roots that exit the spinal column. The target during an epidural procedure is this fluid-filled channel, rather than a specific joint capsule. Navigating these two zones requires different clinical approaches, needle gauges, and entry angles.
Anatomical targets also dictate the distribution of the injected medications. A facet injection remains localized within the joint capsule or around the medial branch nerves that transmit pain signals from that specific joint. An epidural injection relies on the diffusion of anti-inflammatory medications throughout the epidural space. This allows the medication to wash over multiple spinal nerve levels. This systemic wash addresses widespread nerve irritation rather than isolated joint dysfunction.
Clinical Indications: When to Choose Facet Injections vs Epidural
Selecting the appropriate spinal intervention requires a comprehensive diagnostic workup. Physicians recommend facet injections for patients suffering from facet joint syndrome. This mechanical condition causes localized, non-radiating neck or back pain. The pain typically worsens when extending or twisting the spine. It also worsens after prolonged periods of inactivity, such as sleeping. Facet arthropathy does not cause motor weakness or sensory deficits in the limbs. This intervention is highly effective for chronic back pain relief when conservative therapies fail.
Physicians reserve epidural injections for patients experiencing radicular pain. Radiculopathy occurs when a spinal nerve root becomes compressed or inflamed. This leads to shooting pain, tingling, or weakness that travels along the nerve pathway into the buttocks, thighs, calves, or arms. Common underlying diagnoses include herniated discs, foraminal spinal stenosis, and degenerative disc disease. Patients experiencing these symptoms often require an epidural injection to target the transforaminal, interlaminar, or caudal spaces.
Identifying the primary source of pain prevents ineffective treatments. For instance, injecting the facet joint of a patient with a herniated disc causing severe sciatica will not relieve their leg pain. Conversely, administering an epidural to a patient with pure mechanical joint arthritis will yield disappointing results. Clinical practitioners use physical examinations, magnetic resonance imaging (MRI), and computed tomography (CT) scans to differentiate between these mechanical and neuropathic pain syndromes.
Efficacy and Expected Outcomes: Epidural vs Facet Injections
The therapeutic longevity and success rates of these two procedures vary based on the underlying pathology and patient compliance with post-injection rehabilitation. Facet joint injections often provide dual benefits. They offer immediate diagnostic feedback from the local anesthetic and long-term anti-inflammatory relief from the corticosteroid. According to a clinical review published by the American Society of Regional Anesthesia and Pain Medicine, facet-mediated pain accounts for approximately 15% to 45% of chronic lower back pain cases, and targeted injections successfully alleviate symptoms in a significant portion of this population.
If a facet injection yields significant short-term relief but the pain returns, it confirms the facet joint as the primary pain generator. This diagnostic confirmation allows the clinician to recommend a more permanent solution, such as radiofrequency ablation of the medial branch nerves. Radiofrequency ablation can disrupt the nerve pathways, providing pain relief for 6 to 18 months. Without the initial diagnostic facet injection, performing radiofrequency ablation is clinically contraindicated.
Epidural injections focus on reducing nerve root inflammation to facilitate natural healing or physical rehabilitation. Data compiled by the North American Spine Society indicates that epidural steroid injections provide significant short-term relief (exceeding 50% pain reduction) in over 70% of patients presenting with acute lumbar disc herniations. This window of pain relief allows patients to actively participate in physical therapy, which is crucial for long-term recovery and stabilizing the spine.
Procedure Protocols for Facet Injections and Epidural Injections
Both spinal interventions are outpatient procedures performed under local anesthesia. Patients remain awake and communicative throughout the process, allowing them to report any unusual sensations, such as sudden neuropathic pain. Both procedures follow a structured, sterile clinical protocol to ensure patient safety and precision.
- The patient lies in a prone (face down) position on a specialized fluoroscopy table, with pillows positioned to optimize spinal alignment.
- The clinical team cleans the target area of the back or neck with an antiseptic solution and drapes it to maintain a sterile field.
- The physician injects a local anesthetic (such as lidocaine) into the skin and underlying tissues to numb the pathway of the procedural needle.
- Using real-time fluoroscopic X-ray guidance, the physician advances a specialized spinal needle to the precise target—either the facet joint capsule or the epidural space.
- The physician injects a small amount of contrast dye to confirm the needle tip is not in a blood vessel and is in the correct space.
- The physician delivers the therapeutic mixture of local anesthetic (such as bupivacaine) and corticosteroid (such as dexamethasone or triamcinolone).
- The clinical team removes the needle, cleans the skin, applies a small sterile dressing, and monitors the patient in a recovery bay for 15 to 30 minutes.
The entire procedure takes 15 to 30 minutes. Patients must arrange for a designated driver to transport them home. This is necessary because the local anesthetic can cause temporary numbness or mild motor weakness in the limbs. Most patients resume their normal, non-strenuous activities the following day.
Risk Profiles of Epidural vs Facet Injection Interventions

While both procedures are minimally invasive and safe, they carry unique risk profiles due to their anatomical targets. Facet injections carry a lower risk of serious neurological complications. The target joints sit on the outer aspects of the spinal column, far from the central spinal cord. The most common side effects of facet injections include localized soreness, temporary muscle spasms, and minor bleeding at the injection site. A localized steroid flare, which temporarily increases pain for 24 to 48 hours, can also occur.
Epidural injections carry slightly higher risks due to the needle’s proximity to the central nervous system. The most common minor complication is a post-dural puncture headache, commonly referred to as a spinal headache. This occurs if the needle accidentally punctures the dura mater, causing cerebrospinal fluid to leak. This headache is typically positional, worsening when standing and improving when lying down. It can be treated with hydration, caffeine, or an epidural blood patch if it persists.
Extremely rare but serious risks associated with epidural injections include epidural hematoma, epidural abscess, and nerve injury. To minimize these risks, physicians utilize advanced imaging, sterile techniques, and non-particulate steroids (such as dexamethasone) in the cervical and thoracic regions. According to safety briefs from the National Institute of Neurological Disorders and Stroke, serious neurological complications occur in fewer than 1 in 10,000 epidural procedures when performed by board-certified specialists using fluoroscopic guidance.
Financial Costs of Facet Joint Injection and Epidural Injection Procedures

The financial costs associated with these spinal interventions vary based on the clinical setting, geographic region, and insurance coverage. Generally, facet joint injections are more expensive than epidural injections. This is because facet procedures often require targeting multiple levels (e.g., L3-L4, L4-L5, and L5-S1) bilaterally to achieve therapeutic efficacy. Each targeted joint incurs additional drug, equipment, and facility fees.
For patients paying out-of-pocket or with high-deductible insurance plans, an epidural injection typically costs between $600 and $1,800. This price range includes the physician’s fee, facility fee, and the cost of the medications and contrast dye. A multi-level bilateral facet joint injection procedure can range from $1,200 to $3,500. Procedures performed in an ambulatory surgical center (ASC) are generally less expensive than those performed in a hospital outpatient department (HOPD).
Most commercial insurance providers, Medicare, and Medicaid cover both procedures. However, they require prior authorization. Insurance carriers typically require documented proof that the patient has completed at least six weeks of conservative treatment. This includes physical therapy, chiropractic care, and oral anti-inflammatory medications. The clinical team must also submit detailed medical records and imaging reports to justify the medical necessity of the intervention.
Comparative Matrix: Facet vs Epidural
| Feature | Facet Joint Injection | Epidural Injection |
|---|---|---|
| Primary Anatomical Target | Facet joint capsule or medial branch nerves | Epidural space surrounding the spinal nerves |
| Primary Type of Pain Treated | Localized, mechanical axial neck or back pain | Radiating, neuropathic arm or leg pain (radiculopathy) |
| Diagnostic Value | High (helps confirm or rule out facet joint syndrome) | Moderate (primarily therapeutic) |
| Typical Cost Range | $1,200 – $3,500 (multi-level) | $600 – $1,800 |
| Common Diagnostic Indicators | Pain with spinal extension and rotation | Positive straight leg raise test, dermatomal sensory loss |
Professional Clinical Recommendations: Avoiding Diagnostic Pitfalls
A common clinical mistake in pain management is misinterpreting referred pain. Facet joint arthritis in the lower lumbar spine can refer pain into the buttocks and posterior thigh. This referred pain closely mimics the radicular pain associated with sciatica or a herniated disc. However, referred facet pain does not travel below the knee and is not accompanied by neurological deficits, such as a loss of deep tendon reflexes or muscle weakness. Treating referred facet pain with an epidural injection is a common clinical pitfall that leads to poor outcomes.
To avoid this diagnostic pitfall, clinicians must perform a comprehensive physical examination. This includes utilizing provocative maneuvers like the Kemp’s test to stress the facet joints and confirm mechanical pain. If the physical exam points to facet arthropathy, a diagnostic facet injection should be the first-line interventional procedure. If the clinical picture is unclear, performing a diagnostic injection with local anesthetic alone can confirm the source of the pain before administering therapeutic corticosteroids.
Additionally, clinicians must avoid over-relying on corticosteroid injections. Repetitive steroid injections within a short timeframe can cause systemic side effects. These include adrenal suppression, osteoporosis, and elevated blood glucose levels. Clinicians should limit spinal steroid injections to a maximum of three to four sessions per year. If a patient does not achieve significant, sustained relief after two injections, the clinical team should re-evaluate the diagnosis and explore alternative therapeutic options.
FAQ
What is the main difference between a facet injection and an epidural injection?
A facet injection targets the small joints connecting the vertebrae to treat localized mechanical back pain. An epidural injection delivers medication to the space surrounding the spinal nerves to treat radiating pain caused by nerve compression.
How do I know if my back pain is coming from my facet joints?
Facet joint pain is typically localized to the spine, worsens with twisting or bending backward, and does not radiate past the knee. A physical examination and a diagnostic facet block can confirm if these joints are the primary source of your pain.
Which injection is more painful to receive?
Both procedures involve a similar level of mild discomfort, which is minimized by using a local anesthetic to numb the skin. Patients typically report a feeling of pressure rather than sharp pain during the injection of the medication.
How long does relief last after an epidural steroid injection?
The duration of relief varies from several weeks to several months, depending on the severity of the nerve compression. This pain-free window is designed to allow patients to participate in physical therapy to address the root cause of their symptoms.
Can I get a facet injection and an epidural injection at the same time?
While it is anatomically possible, clinical guidelines generally advise against performing both injections in a single session. Combining the procedures makes it difficult to determine which injection provided relief, which complicates future treatment planning.
Is a referral required to get these spinal injections?
Most insurance plans and specialists require a referral from a primary care physician, chiropractor, or physical therapist. This referral ensures that conservative treatment options have been explored and that a preliminary diagnostic assessment has been completed.